
Epidermal nevi are overgrowths or hamartomas of epidermal cells, which have a genetic basis. They are due to mosaic somatic mutations which lead to proliferation of one or other component of the epidermis.
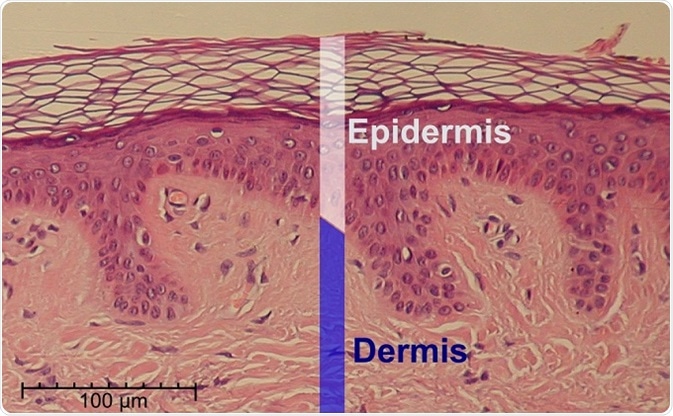
A hematoxylin and eosin stained slide of normal epidermis and dermis.
Types of epidermal nevi
Epidermal nevi are grouped by their clinical features, by the site of occurrence, and their extent of spread, but mostly by which epidermal cell predominates in the lesion. In some patients, multiple epidermal nevi occur along with systemic abnormalities and they form the epidermal nevus syndromes.
Based on their patterns of occurrence, epidermal nevi are named differently despite a similar microscopic appearance:
- Nevus verrucosus: occurs as a single lesion or multiple lesions but always localized
- Nevus unius lateris: a linear pattern of lesions is seen
- Ichthyosis hystrix: generalized lesions are present
Epidermal nevi are also classified by their cell of origin:
Nevus sebaceous
Sebaceous nevi are quite common, and are made up of sebaceous glands with or without hair follicles. They are found commonly on the scalp but also on the trunk or extremities. They are pale yellow in color, with a smooth hairless surface. They are present in young babies though they may manifest only after puberty or in childhood. About a fourth of them eventually give rise to tumors, mostly benign. It is associated with the occurrence of Schimmelpenning syndrome, phakomatosis pigmentokeratotica, didymosis aplasticosebacea, and SCALP syndrome.
Keratinocytic epidermal nevus
These are also called non-organoid epidermal nevi, and are quite common among this group of lesions. They follow the lines of Blaschko. Beginning as brownish macules, they thicken and darken with age to become plaques. They may be described as linear or verrucous, based on their appearance. Other variants include the epidermolytic epidermal nevus; the acantholytic epidermal nevus; and the systematized epidermal nevus.
Epidermal nevi are often associated with mental retardation, bone anomalies, and strabismus. Various ENS have been reported with these lesions, such as Proteus and CHILD syndrome, and type 2 segmental Cowden disease.
Nevus comedonicus
These lesions are formed of proliferated dilated keratinized follicles, often inflamed or showing signs of infection. They are the result of blockage, forming blackheads, and pitting is often seen. It may be associated with brain abnormalities, bone defects, and cataracts.
Angora hair nevus
The Angora hair nevus is an epidermal nevus which is remarkable for the long and soft white hair, like Angora wool, that grows from it. It may be associated with other defects of the brain and bones.
Becker nevus
The Becker nevus is a dark patch of hairy skin appearing to have a checkerboard shape, becoming larger and darker after puberty because of its androgen-dependent nature. It is found more frequently on the upper part of the back or the shoulders. It is associated with other skeletomuscular defects, forming the Becker nevus syndrome.
Inflammatory linear verrucous epidermal nevus
This type of epidermal nevus is linear and forms plaques, usually unilateral. They are usually pruritic, and appear inflamed and hyperkeratotic. The first appearance is after six months of age. Some patients may have bone anomalies as well.
Porokeratotic eccrine nevus
This type of epidermal nevus appears as warty keratotic papular lesions, mostly on the palms and soles, but in some cases they may appear all over the skin.
References
- https://patient.info/doctor/epidermal-naevus-and-its-syndromes
- https://www.ncbi.nlm.nih.gov/pubmed/20875335
- http://www.dermnetnz.org/topics/epidermal-naevus-syndromes/
- https://rarediseases.org/rare-diseases/epidermal-nevus-syndromes/
- https://ghr.nlm.nih.gov/condition/epidermal-nevus
Further Reading
- All Epidermal Nevus Content
- Epidermal Nevus Overview
- Epidermal Nevus Treatment
- Epidermal Nevus Syndromes
- Complications of Epidermal Nevi
Last Updated: Feb 26, 2019

Written by
Dr. Liji Thomas
Dr. Liji Thomas is an OB-GYN, who graduated from the Government Medical College, University of Calicut, Kerala, in 2001. Liji practiced as a full-time consultant in obstetrics/gynecology in a private hospital for a few years following her graduation. She has counseled hundreds of patients facing issues from pregnancy-related problems and infertility, and has been in charge of over 2,000 deliveries, striving always to achieve a normal delivery rather than operative.
Source: Read Full Article