
A distinguishing feature of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) compared to severe acute respiratory syndrome (SARS) is that it is spread not only via symptomatic people but also asymptomatic and pre-symptomatic people. Asymptomatic cases are becoming of increasing concern due to the potential of people unknowingly causing local outbreaks within their communities. In response to this public health risk, numerous studies have been performed to understand the mechanism of asymptomatic infection with SARS-CoV-2.
 Study: Asymptomatic SARS-CoV-2 infection and the demography of COVID-19. Image Credit: TierneyMJ/ Shutterstock
Study: Asymptomatic SARS-CoV-2 infection and the demography of COVID-19. Image Credit: TierneyMJ/ Shutterstock
The studies conducted to review the state of asymptomatic infection have reported the proportion of cases to vary between 1.21% and 91.88%; when age stratification is applied to asymptomatic cases, a substantial variation is observed according to age. This suggests that local demography could be integral in observed geographical and age-related heterogeneity of asymptomatic case proportion.
Testing bias, measurement of asymptomatic status, and sampling bias are the main obstacles to navigating to understand better the heterogeneity associated with asymptomatic cases. Due to passive surveillance mainly being limited to symptomatic cases, a large proportion of asymptomatic expected to go unreported.
The study
In a study available on the preprint server medRxiv*, data was collected from six cities within China to investigate how asymptomatic infection varied by age and geographic location. There were 2,744 cases of coronavirus disease 2019 (COVID-19) confirmed by PCR test with the highest number of cases from Shijiazhuang (1.040) and the lowest number of cases from Xingtai (80). The distribution of infection varied by age in each location, with the largest proportion of positive cases identified in people aged >60 in Shijiazhuang, Suihua, Tonghua, and Changchun and 40-49 in Harbin.
A wide variation was observed in asymptomatic cases, with 8% in Tonghua, 18% in Shijiazhuang, and 51% in Harbin. Due to the populations being tested multiple times during outbreaks and the identified cases were isolated and under 14-days health monitoring to create a definite clinical outcome per individual, there should only be a very small bias in this asymptomatic proportion calculation. Within the six cities, the proportion of asymptomatic infections declined with age.
Some studies have reported that the risk of being symptomatic with COVID-19 is significantly reduced when individuals are vaccinated. However, due to the vaccine rollout starting after this data was collected, it is unlikely that vaccinations contributed to the heterogeneity displayed in asymptomatic people. Exposure during the first wave of the pandemic in which antibodies would have been produced against SARS-CoV-2 is also unlikely to have contributed to heterogeneity because, within the six cities, the number of infections was relatively small.
The authors hypothesized that the six cities reported different proportions of SARS-CoV-2 infections because of the age distribution of infections, the interplay between the age-dependent asymptomatic proportion of cases, and the age distribution of the underlying susceptible population.
To examine their hypothesis, the authors designed an age-stratified discrete stochastic compartment model that incorporated age-dependent asymptomatic proportions to reconstruct observed epidemic trajectories, including both symptomatic and asymptomatic cases.
The model suggested that if the proportion of asymptomatic cases had been equal across all age groups, the total number of asymptomatic cases in each city would have been the same. However, this was contradicted by the observations, which show that asymptomatic proportion is age-dependent.
The vaccine rollout has begun for adults, but the future epidemic trajectories are unclear even when all adults are vaccinated. The authors simulated a scenario in which all adults were vaccinated, but children were not, to imitate possible future epidemic trajectories. This scenario showed that even when all adults are fully vaccinated, possible flare-ups of symptomatic COVID-19 within the younger population are possible.
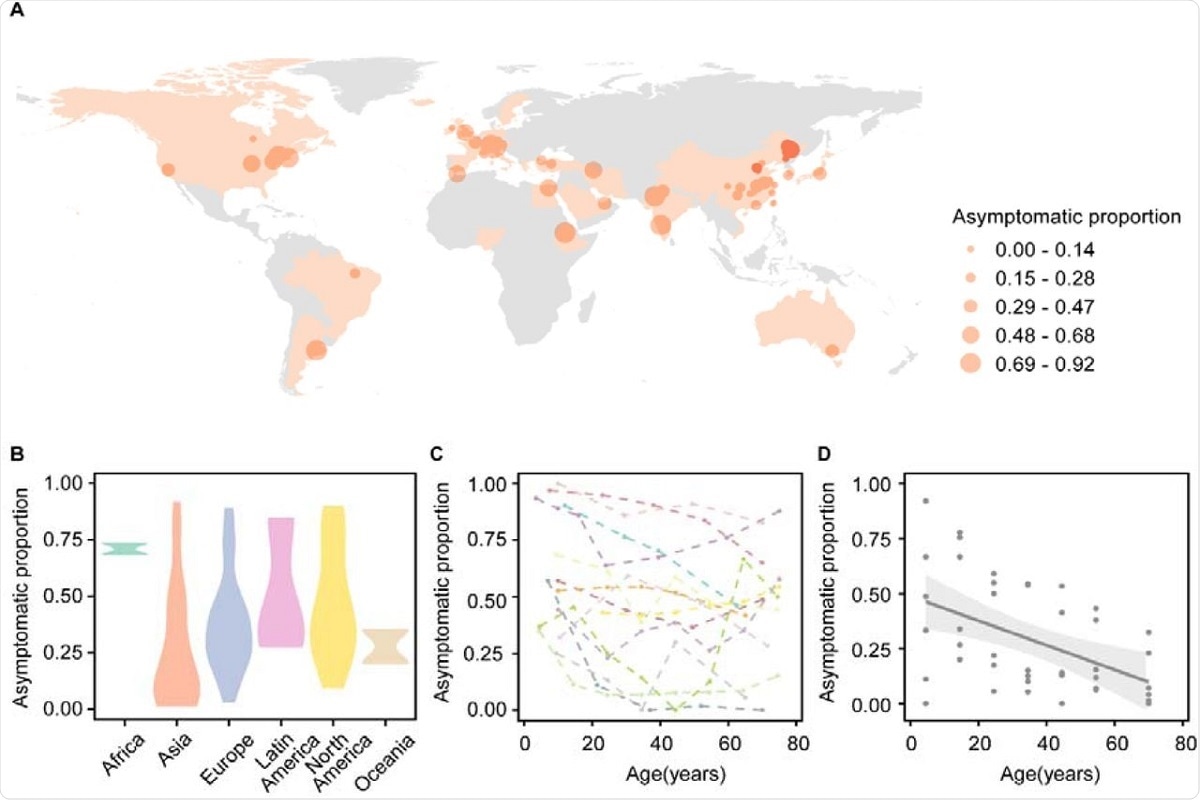 Figure 1. The asymptomatic SARS-CoV-2 cases in the world. (A) The dots on the maps indicate the location of the reported asymptomatic proportions. The dot size indicates the asymptomatic proportion. The red dot represents the data in our study. (B) The violin plot for the reported asymptomatic proportion in the continents. (C) The asymptomatic proportion reported by age in previous studies. (D) The grey points represent the data from Chinese cities. A linear regression was built (Asymptomatic proportion = Intercept+Coeffecient×Age). The grey line represents the linear regression using pooled asymptomatic proportion under each age group across cities with 95% CI in light grey shadow (Coefficient=-0.006, P-value<0.01). To get a reliable estimate, only the asymptomatic proportions derived from more than 50 samples are plotted. Note that the testing methods and definition of asymptomatic cases in these studies were different from ours. The asymptomatic proportion from other parts of the world may not be comparable to our data directly.
Figure 1. The asymptomatic SARS-CoV-2 cases in the world. (A) The dots on the maps indicate the location of the reported asymptomatic proportions. The dot size indicates the asymptomatic proportion. The red dot represents the data in our study. (B) The violin plot for the reported asymptomatic proportion in the continents. (C) The asymptomatic proportion reported by age in previous studies. (D) The grey points represent the data from Chinese cities. A linear regression was built (Asymptomatic proportion = Intercept+Coeffecient×Age). The grey line represents the linear regression using pooled asymptomatic proportion under each age group across cities with 95% CI in light grey shadow (Coefficient=-0.006, P-value<0.01). To get a reliable estimate, only the asymptomatic proportions derived from more than 50 samples are plotted. Note that the testing methods and definition of asymptomatic cases in these studies were different from ours. The asymptomatic proportion from other parts of the world may not be comparable to our data directly.
Implications
This study highlights how COVID-19 outbreaks may occur from mostly asymptomatic, susceptible, and unvaccinated young age groups. Control measures may need to be implemented among the younger age groups to avoid resurgence within the population. In addition, the study provides insights into the observed variability in the proportion of asymptomatic SARS-CoV-2 infections.
Previous research and the data presented in this study underpin the proportion of asymptomatic cases as a non-increasing function of age. However, future research is required to fully understand what changes may occur in asymptomatic proportions with accumulated natural exposure, the emergence of new variants, and immunity induced by imperfect vaccines.
*Important notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- Wang, Z. et al. (2021) "Asymptomatic SARS-CoV-2 infection and the demography of COVID-19". medRxiv. doi: 10.1101/2021.09.03.21262757.
Posted in: Medical Science News | Medical Research News | Disease/Infection News
Tags: Antibodies, Children, Coronavirus, Coronavirus Disease COVID-19, immunity, Pandemic, Public Health, Research, Respiratory, SARS, SARS-CoV-2, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, Syndrome, Vaccine

Written by
Colin Lightfoot
Colin graduated from the University of Chester with a B.Sc. in Biomedical Science in 2020. Since completing his undergraduate degree, he worked for NHS England as an Associate Practitioner, responsible for testing inpatients for COVID-19 on admission.
Source: Read Full Article